
You might be wondering what, exactly, I mean by this question. Value-based care has been the strategy of choice for health care’s new entrants over the past decade-plus. Not eager to be left behind, and given government incentives to provide this type of care, many incumbents have attempted to implement similar strategies—usually with limited success. We are now seeing a similar industry-wide fervor around vertical integration as a popular strategy to employ.
But is the hype warranted?
Is vertical integration really the winning strategy to improve health and health systems’ bottom lines? It’s unlikely for a variety of reasons, and I’ll explain why through three theory-based lenses.
1. Business models depend on an organization’s context, and they solidify over time
Strategies and business models are not one-size fits all.
Business models determine an organization or company’s capabilities (what it can and can’t do) and its priorities (what it must accomplish). This, in turn, defines which innovations it can and will pursue. The business model framework is powerful because it enables the prediction of which initiatives will succeed and which ones will fail.
An organization’s context—including its vision, mission, and beliefs about the future—are critical inputs to crafting and executing a successful business model. As the term “business model” is often misunderstood, the Christensen Institute has a framework to make this potentially nebulous concept clear. Below, in Figure 1, you can see the four components of a health care business model. Once business models are solidified, they are increasingly resistant to change—in both health care and other industries. I’ve written about this concept before, and why business models operate this way.
Figure 1. The four components of a health care business model
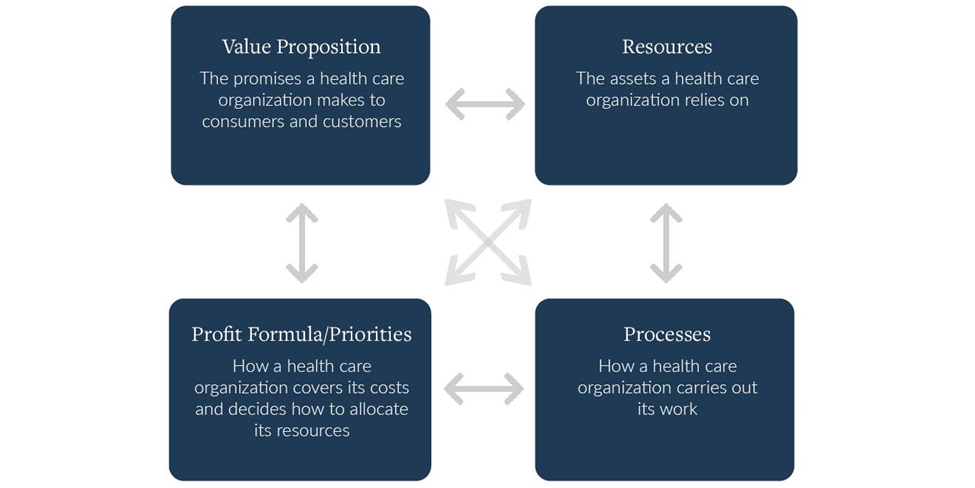
Note: This graphic was originally published by Clayton M. Christensen and Mark W. Johnson, “What Are Business Models, and How Are They Built?” Harvard Business School Module Note, August 2009 (revised November 2021). It has been modified to focus on health care business models.
To survive infancy, organizations pivot their value propositions and adjust their resources and processes until they identify how to bring in the revenue they need to survive. Once this is determined, business model components become increasingly interdependent and resistant to change, especially in successful organizations. The ways in which the four components reinforce one another makes the business model highly interconnected, and thus more challenging to alter the longer it exists. In short, business models solidify over time.
For a deeper dive on why an individual entity’s context is critical and how to identify the right strategy and associated business model for an organization, see our report on this topic: Improve or transform. In it, executives will find a strategy primer and decision tool to help them determine the best strategy for their organization, based on their current and projected future contexts.
2. Organizations seeking to employ vertical integration strategies aren’t in their infancy
Incumbent health systems, such as The Cleveland Clinic and Advocate Health, as well as new entrants to health care provision, such as CVS and Walgreens, are not new business models. These organizations have been around for multiple decades in some cases, and over a century in others. As a result, their business models are hardwired to operate in a way that reliably delivers on their value proposition.
However, none of these organizations started as vertically-integrated business models providing the full continuum of health care services. Instead, they started as multi-specialty groups, hospitals, or pharmacies. As a result, executing the strategic shift from any of these businesses to a vertically-integrated health care services firm requires a complex business model transformation. As we detail in Improve or transform, such a transformation is not a small undertaking.
Kaiser is a notable example where the integration of competing insurance and care provision business models has worked. But, as discussed in a recent piece on The Health Care Blog, Jeff Goldsmith argues this is likely due to the market conditions in Kaiser’s original market as opposed to its vertical strategy. Business model theory would posit that their success is also due—at least in part—to the fact that vertical integration was a key part of their original business model.
So, yes, context is critical. And altering one’s original business model to serve multiple, divergent customer value propositions is increasingly difficult as time goes on and as the number of value propositions one attempts to serve increases.
3. Vertical integration requires one to run various types of business models under one umbrella
Goldsmith notes that the concept of vertical integration arose from the industrial economy, yet, the health care value chain is “fundamentally different and more complex than that in manufacturing or retailing.” As a result, one cannot apply a strategy from industrial value chains to an industry built upon trust and relationships. It’s also a risky strategy because of the different types of business models involved.
There are three distinct types of business models (see Figure 2). And operating various types under one umbrella organization is a challenging feat due to the different resources, processes, priorities, and profit formulas required to deliver on various value propositions. The three types are as follows:
- Solution shops: Resources and processes are set up to diagnose and recommend solutions to complicated problems. These businesses are typically paid through a fee-for-service revenue model because paying based on outcomes depends on too many other factors outside of the quality of their recommendations.
- Value-adding process shops: These business models bring in incomplete ingredients and then add value to them before delivering them to the customer. These businesses have a fee-for-outcome revenue model.
- Facilitated networks: In these models, the same people buy and sell or deliver and receive things from each other. Companies that make money in these industries are the ones that facilitate the effective operation of the network. Social media companies are examples.
Figure 2. Three types of business models

In a vertical integration strategy, one must execute all three types of business models at once. This is unlikely to succeed. As Christensen outlines in The Innovator’s Prescription, “The general hospital is not a viable business model…The value proposition, which is to diagnose and treat any disorder that anyone might bring through their doors, has caused them to harbor each of the three generic types of business models under the same roof…Hospitals need to disrupt themselves into the three types of business models, or they must be disrupted by others.”
As health systems continue down the vertical integration pathway, and new entrants attempt to do the same, it begs the question: Why repeat the business model design error that has led to financial hardships, slim and tightening margins, and declining health outcomes? Business model theory suggests this is not the best strategic choice one could make to promote business model viability.
Conclusion
Much like the shift to value-based care was perhaps over-hyped because of the difficulty of transforming entrenched business models en-masse, we are apt to see a similar outcome with the currently popular strategy of vertical integration.
It’s not that vertical integration is a “bad idea” or a “bad strategy,” because strategic fit depends on one’s context. But as business model theory suggests, it’s not a one-size-fits-all strategy for success. This is especially true in health care, where a vertical integration approach necessitates that one run various types of business models under one roof.
In short, if you decide to wade into the vertical integration waters, keep these three factors in mind, and tread wisely.

