
Maternal health in the US is in a severe state. If you’re reading this, you’re likely familiar with the statistics. In brief, despite spending more money per capita on maternity care than any other country, the US has worse maternal health outcomes than all high-income countries.
There have been multiple rallying cries to do something about this horrific status quo. Perhaps most influential among them was the CDC’s 2022 report, which stated over 80% of these deaths were avoidable. Additionally, the problem is worse for birthing people of color.
Pause for just a minute and think about that statistic.
Over 80% of maternal deaths were avoidable.
That means if ten people died as a result of pregnancy or postpartum complications, at least eight could still be alive today if better care practices were in place.

Policies are a critical lever for change. But as I’ll detail here, policy alone is not enough.
What is Transforming Maternal Health?
In December, CMS announced its new effort to improve maternal health outcomes: The Transforming Maternal Health (TMaH) Model. The announcement detailed that CMS will issue awards for up to 15 states where State Medicaid Agencies (SMAs) will receive up to $17 million in funding for a ten-year period. States are required to implement certain elements of the TMaH model to receive the payments. These include the following, among other things:
- Perform risk assessment, referral, and follow-up for perinatal depression, anxiety, tobacco, substance use, and health-related social needs (a.k.a. drivers of health)
- Provide home monitoring of diabetes and hypertension
- Develop a health equity plan
- Provide access to midwives, birth centers, and coverage for doulas
- Improve data infrastructure and payment models
- Implement patient safety protocols and promote “Birthing-Friendly” designation
Coverage of evidence-based services and implementation of these stated capabilities is a great start. But it’s truly just a start. For example, including social needs assessments and referrals is good, but as detailed in our research report, You are what you treat, this isn’t sufficient to improve health outcomes. An entity must have a supportive business model in place to move the lever. (See the report for the types of business models that do this effectively.)
Additionally, home monitoring, a health equity focus, coverage of midwifery and doula services are also great investments that demonstrate a willingness to put evidence-based practices in place. For example, we know access to doula care—both virtual, and in-person—improves health outcomes.
But, as a nation, we must do more to achieve the goal of reduced maternal mortality. The Tools of Cooperation framework details why this is the case.
Tools of Cooperation: A brief primer
How can leaders convince individuals to cooperate and work together? There are a variety of tools, ranging from motivational, visionary speeches to command-and-control orders that a leader can use to elicit cooperative behavior. These are called the Tools of Cooperation (ToC).
The first important thing to know is that most of these tools don’t work most of the time.
As a result, leaders often fail when trying to manage change, since the tools they use waste credibility, energy, and resources. Therefore, the most important upfront action is to assess one’s circumstance in terms of stakeholder agreement on what the goals of the society should be and how it can achieve them.
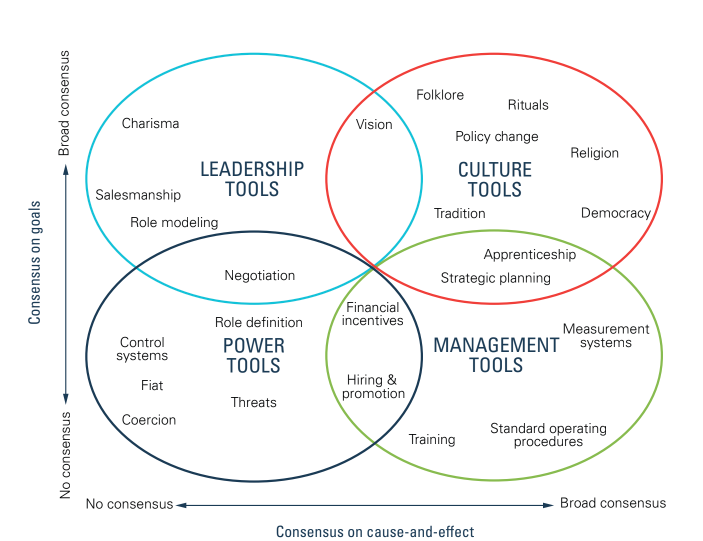
Figure 1 depicts these two variables. The vertical axis measures the extent to which the people involved agree on the goals. In other words, what do they want? This incorporates the results they seek from being part of the community, to what their values and priorities are, to which trade-offs they are willing to make to achieve those results. The extent of agreement can range from none (at the bottom) to complete agreement (at the top).
The second dimension is plotted on the horizontal axis. It measures the extent to which the people involved agree on cause and effect—which actions will lead to the desired result. In other words, how will we achieve our goals? On the right-hand side, strong agreement on cause and effect implies a shared view of the processes that should be used to get any particular outcome, whereas little agreement on cause and effect places a society or organization on the left-hand side of the diagram.
Figure 1. The Tools of Cooperation
Leaders seeking a specific change will find that figuring out their constituents’ placement on this diagram is time well spent. Getting the diagnosis right has profound implications for how to roll out any proposed change.
Tools of Cooperation applied to maternal health
As a nation, thanks to many advocacy efforts over the past few years, there is fairly broad consensus that as the world’s wealthiest nation, it’s unacceptable to have the highest maternal mortality rate, as well as the highest percentage of avoidable maternal deaths. Therefore, one could say we are broadly aligned around a goal of reducing pregnancy and postpartum-related deaths. This places us in the upper half of the ToC framework.
However, there has not been, and is not yet, broad consensus on the cause-and-effect, that is to say how we can reduce maternal deaths. CMS’s policy change shows that we are gaining consensus on the cause-and-effect axis, as demonstrated by the fact that the policy has been enacted. What is still unclear is if the policy change will be effective at lowering mortality rates.
A way forward through policy and…
As a result, and as I noted in a previous piece, investments by large employers play a key role in bolstering this consensus. Given the timeline for CMS’s investment (implementation of the TMaH model starts in 2028), it’s critical that large employers continue to leverage the Leadership Tools at their disposal, such as role modeling, in order to build momentum at the societal level and continually push us towards a quadrant where we not only have broader agreement on how to achieve the goal of reduced maternal mortality, but also to a place where policy change is more effective. What Walmart is doing is a great example of employer leadership.
The ToC framework provides support for what we inherently know to be true: to solve a problem as large as 80% of maternal deaths being avoidable, we need support and leadership from all corners of society. That means we need government and business leaders to leverage the tools at their disposal to help shift us toward broad consensus on “how” to reduce maternal mortality.
So while policy change is a critical lever to pull, it isn’t the only one. And with a 2028 start date, it definitely isn’t the fastest. Waiting until 2028 for improvement means four more years of mothers dying unnecessarily. When it comes to consensus, I think we can all agree that’s completely unacceptable.

